
An important Life for a Child / University of Pittsburgh study showing how low-income countries can reduce the rate of complications from type 1 diabetes (T1D) has been published by the academic journal Pediatric Diabetes. Young people supported by Life for a Child live in in low- and middle-income countries with competing priorities for healthcare spending. Some governments only provide one component of care for their young citizens living with T1D (such as insulin) and many don’t provide anything at all.
“Consequently, the kinds of care that are offered to those with type 1 diabetes in these countries is often at a ‘minimal’ level. The bleak outcomes of this level of care include high mortality and the premature onset of devastating and costly chronic complications.” Dr. Graham Ogle, General Manager Life for a Child.
In order to support our local partners in their efforts to advocate for more government help for children with diabetes, we set out to demonstrate how effective even modest improvements in care provision can be.
We did this by looking at the costs and outcomes of diabetes care in six countries- Mali, Tanzania, Pakistan, Bolivia, Sri Lanka and Azerbaijan.
Specifically, we looked at the outcomes for young people receiving minimal and intermediate care. Minimal care was defined as twice daily human insulin injections with no self-blood glucose monitoring and minimal diabetes education. Intermediate care consists of multiple daily insulin injections, two to four blood glucose tests per day, diabetes education and HbA1c testing. For a comprehensive look at these definitions look at our 2018 study into levels of care.
Using a mathematical model we calculated the rate of a range of complications at different HbA1c levels over a 30-year period.
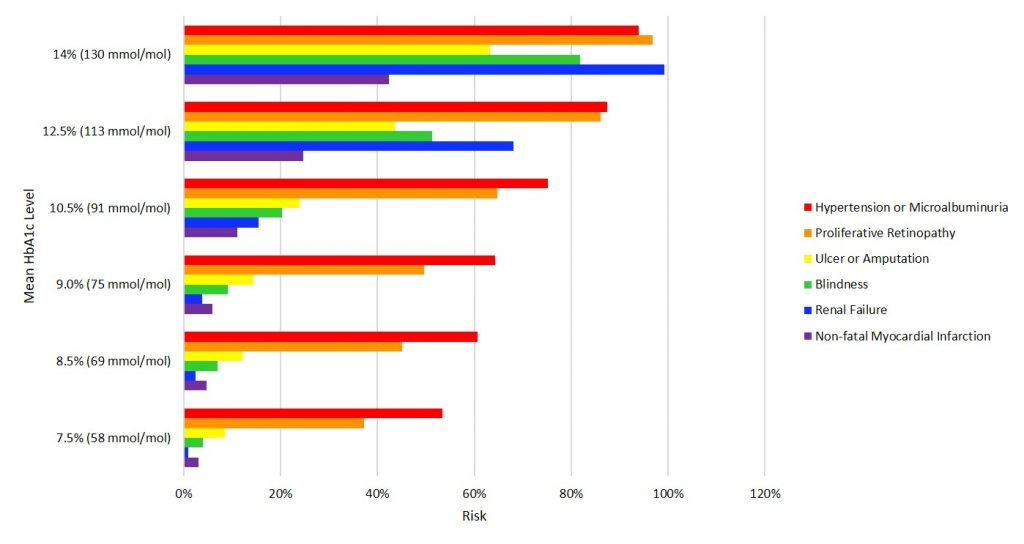
Mathematical modelling: Complications rates after 30 years
The graph above shows the 30-year complications rates at differing mean HbA1c levels, demonstrating the importance of reducing HbA1c.
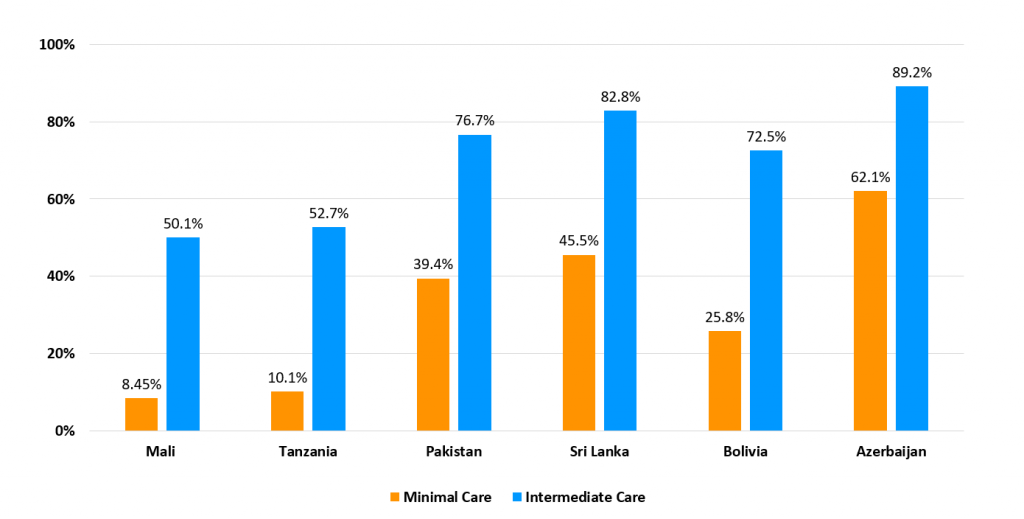
The difference in chance of survival in each country depending on whether the young person is receiving ‘minimal’ or ‘intermediate care’.
As you can see, incidences of complications were lower for young people receiving intermediate care vs. minimal care. Intermediate care is the type supported by Life for a Child.
The study goes on to show that, although intermediate care is a little more costly to maintain than minimal care, acute and chronic complication costs are reduced and young lives are saved. This is a compelling argument for governments to increase provision of care for young people living with T1D.
Dr. Ogle is hopeful that the study will help to improve care: “Overall, these findings could greatly strengthen local efforts made by health care professionals, policymakers and advocates, who are working toward provision of acceptable type 1 diabetes care by their national health systems.”
View the study in Pediatric Diabetes or email us to request a copy at [email protected].